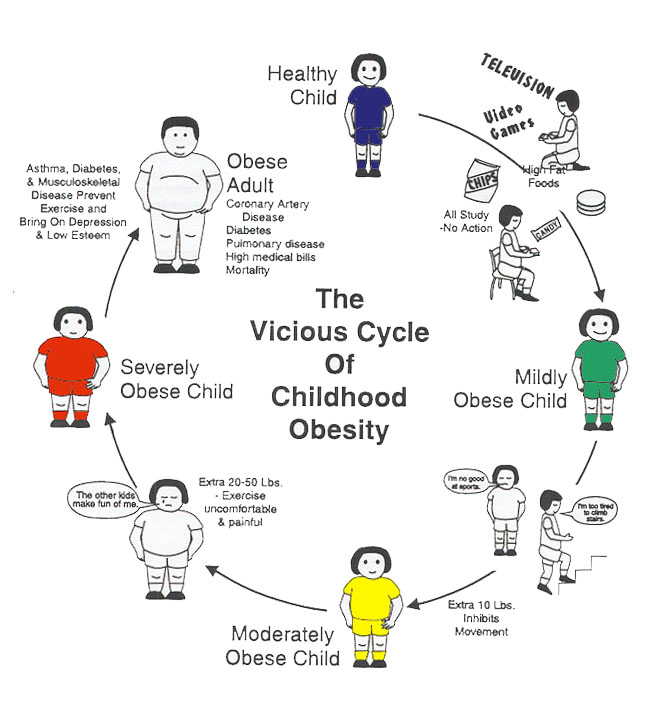
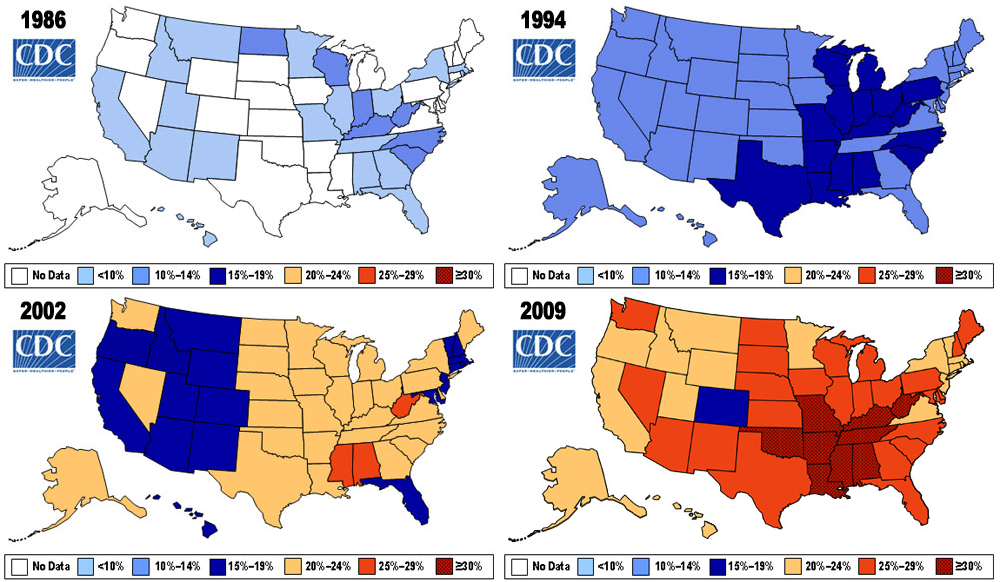
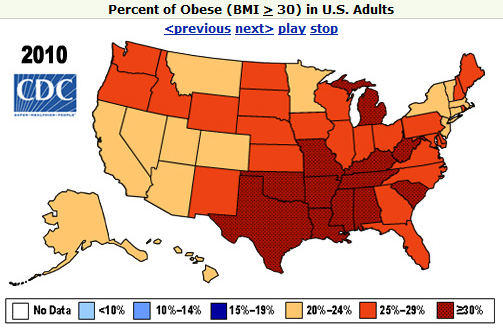
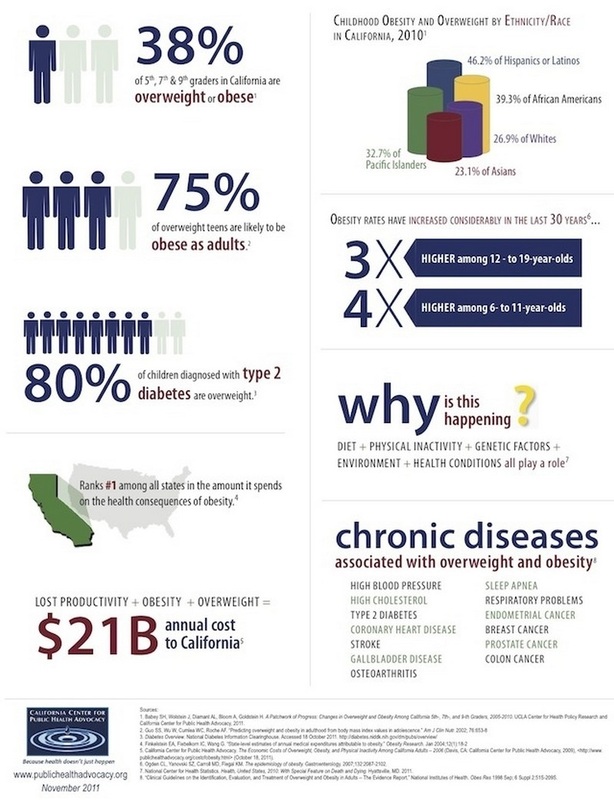
Higher sugar intake increases risk of obesity.
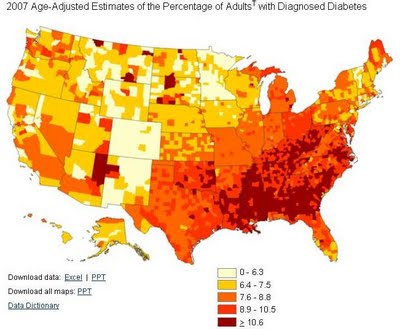
Obesity in turn increases risk for diabetes.
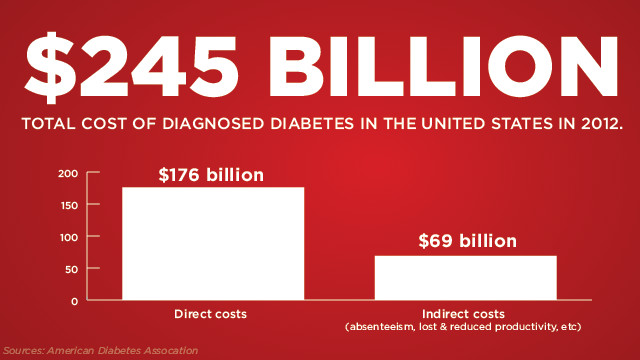
Diabetes can bankrupt the healthcare system.
Obesity in turn increases risk for diabetes.
Diabetes can bankrupt the healthcare system.
|
|
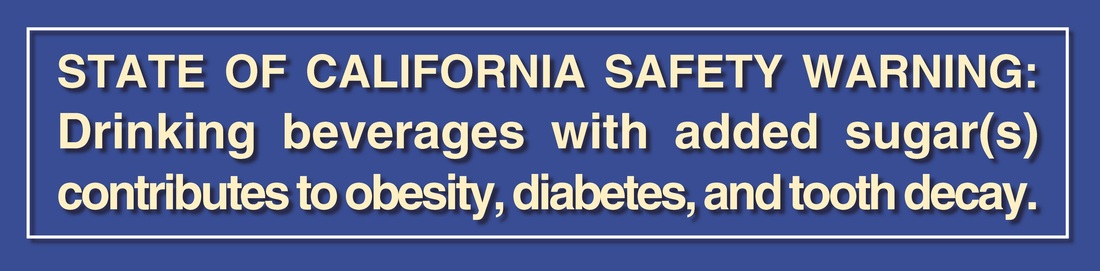
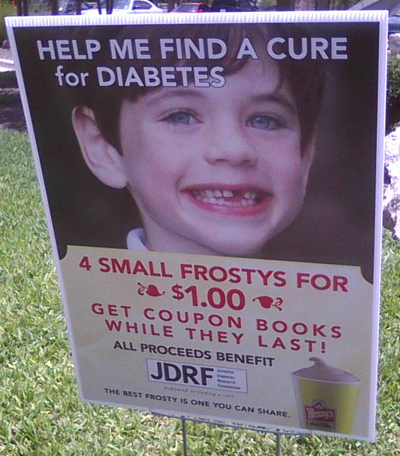
A warning label reminds us the choice comes with risks.
|

|
Warning labels can promote change in both people and the manufacturing industry.

|

Harold Goldstein, CCPHA Director
|
|


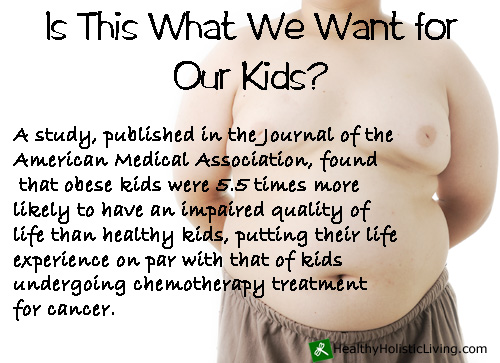
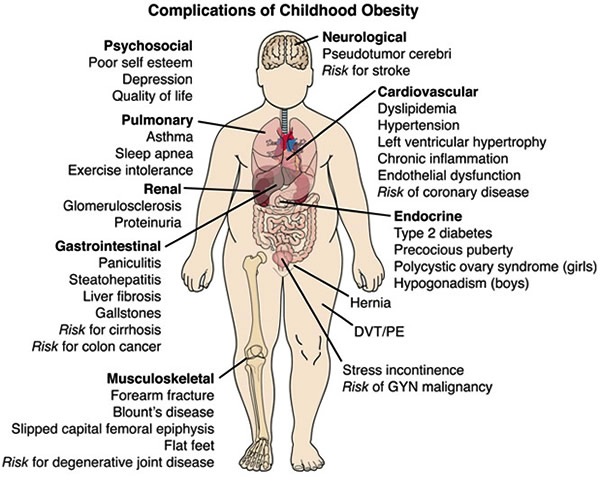
When we think of a child that has been diagnosed with cancer we know that it could be a life and death situation, but do we realize that an obese child could be living with the same fear and not know what to do about it. The California Center for Public Health Advocacy (CCPHA) know from the latest research that liquid sugar such as high frutose corn syrup (HFCS) is a major contributor to childhood obesity. Type II diabetes was a middle aged man disease and now children are being diagnosed with what could be a death sentence in their mind, make them feel labeled, different, ashamed.
The newest diabetes drugs are making it easier and easier to be obese and control your diabetes instead of more healthcare programs that help to reverse the condition with healthy food choices and exercise. Where Type I diabetics have had permanent damage done to the hormone producing glands in the pancreas, the high body fat in the obese Type II diabetic patient is influencing how many insulin receptors are available on the outside of cells.
Once an insulin cell finds a cell docking station it is like a lock and key so the door is open for insulin to come into the cell. The key to unlock the door and allow glucose to go from the blood to inside the cell, kind of like putting the gas nozzel in the gas tank of you car which opens the way for the gas to freely fill the tank with fuel to power the engine and keep self cleaning systems in place and working to rid the body of toxic waste.
Helping the glucose get out of the blood and into your bodies cells not only reduces your overall blood sugar concentrations, but gives your cells the fuel they need to do their job, fuel cell function. When the sugar stays it the blood it becomes concentrated and can easily eat away at thin, vulnerable tissues like those found in the eyes (retinopathy), kidneys (retinopathy), the tips of our fingers and toes (neuropathy), and increases the risk for other of the top killing diseases such as heart disease, stroke/high blood pressure/the silent killer, and cancer. Diabetes is also the #1 cause of amputations.
The cost of a lifetime of diabetes is with the estimate that diabetes will comsume the entire healthcare budget by 2030.
TYPE II DIABETES IS PREVENTABLE
The newest diabetes drugs are making it easier and easier to be obese and control your diabetes instead of more healthcare programs that help to reverse the condition with healthy food choices and exercise. Where Type I diabetics have had permanent damage done to the hormone producing glands in the pancreas, the high body fat in the obese Type II diabetic patient is influencing how many insulin receptors are available on the outside of cells.
Once an insulin cell finds a cell docking station it is like a lock and key so the door is open for insulin to come into the cell. The key to unlock the door and allow glucose to go from the blood to inside the cell, kind of like putting the gas nozzel in the gas tank of you car which opens the way for the gas to freely fill the tank with fuel to power the engine and keep self cleaning systems in place and working to rid the body of toxic waste.
Helping the glucose get out of the blood and into your bodies cells not only reduces your overall blood sugar concentrations, but gives your cells the fuel they need to do their job, fuel cell function. When the sugar stays it the blood it becomes concentrated and can easily eat away at thin, vulnerable tissues like those found in the eyes (retinopathy), kidneys (retinopathy), the tips of our fingers and toes (neuropathy), and increases the risk for other of the top killing diseases such as heart disease, stroke/high blood pressure/the silent killer, and cancer. Diabetes is also the #1 cause of amputations.
The cost of a lifetime of diabetes is with the estimate that diabetes will comsume the entire healthcare budget by 2030.
TYPE II DIABETES IS PREVENTABLE
|
|
|
|
|


|
|

|

The California Center for Public Health Advocacy uses a combination of seven key strategies to build and support policy reforms at the state and local levels. Using these strategies, we have led some of the most successful and groundbreaking obesity prevention campaigns in the country. We also train organizations to use these strategies to support policy reforms addressing these and other public health issues.
I. Community Mobilization. We provide opportunities for individuals and organizations to share their perspectives with policy makers about the need for policy reforms. We also bring advocates and policy makers together to work toward common policy objectives.
II. Research. We publish Policy Briefsand other materials describing health issues related to eating and physical activity and recommending specific policies to address these issues. These materials provide the general public, policy makers and other decision-makers, and advocates with tools to inform the policy development process.
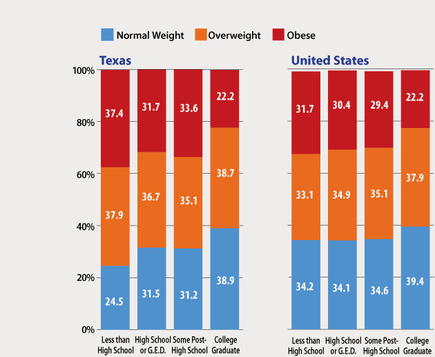
III. State and Local Data. Our Policy Briefs often describe health-related data by city, county, and/or state legislative district to help policy makers, their constituents, local advocates, and the media more fully understand how health issues affect their communities.
IV. Scientific Advisory Panels. We establish scientific advisory panels to assist us in developing policy recommendations included in our Policy Briefs.
V. Media Advocacy. We work with an award winning public relations firm and with local spokespersons to ensure that our message receives as much media attention as possible.
VI. Policy Maker Education. We develop relationships with state and local policy makers and educate local elected officials about the importance of establishing policies to promote healthy eating and physical activity. We provide state and local elected officials with personalized data and technical assistance to help them develop needed policy reforms.
VII. Partnership Building. In nearly all of our work, we build extensive partnerships across different disciplines because we know that partnership building—with local advocates, policy makers, funders, and health, education, social service and other organizations—is often the most critical component in building momentum toward policy change.
I. Community Mobilization. We provide opportunities for individuals and organizations to share their perspectives with policy makers about the need for policy reforms. We also bring advocates and policy makers together to work toward common policy objectives.
II. Research. We publish Policy Briefsand other materials describing health issues related to eating and physical activity and recommending specific policies to address these issues. These materials provide the general public, policy makers and other decision-makers, and advocates with tools to inform the policy development process.
III. State and Local Data. Our Policy Briefs often describe health-related data by city, county, and/or state legislative district to help policy makers, their constituents, local advocates, and the media more fully understand how health issues affect their communities.
IV. Scientific Advisory Panels. We establish scientific advisory panels to assist us in developing policy recommendations included in our Policy Briefs.
V. Media Advocacy. We work with an award winning public relations firm and with local spokespersons to ensure that our message receives as much media attention as possible.
VI. Policy Maker Education. We develop relationships with state and local policy makers and educate local elected officials about the importance of establishing policies to promote healthy eating and physical activity. We provide state and local elected officials with personalized data and technical assistance to help them develop needed policy reforms.
VII. Partnership Building. In nearly all of our work, we build extensive partnerships across different disciplines because we know that partnership building—with local advocates, policy makers, funders, and health, education, social service and other organizations—is often the most critical component in building momentum toward policy change.
|

|

|

|
|
|
|
|
|

|

|
|
|
|
|
|






