|
|
|
Phthlates, GMOs, antibiotics, and other chemicals in cosmetics, air fresheners, cleaners, parfumes, shower curtains, baby, water, and beverage bottles, are making us fat!

|

|

|
|
When I saw the article below, "UnneCesareans: Documented Causes of a Disturbing Trend," I realized that this trend of unnecessary cesareans has not decreased since I had my first baby 26 years ago at home with a midwife.
There are those that choose surgery for convenience and to avoid a vaginal birth, and then there are those that get sucked into the high profit margin surgery whether they need it or not. According to the statistics in the article one in 3,000 die from the surgery. Could understand these numbers if all those in this group started off as "high risk" and therefore would be expected to have higher fatality #'s than the general population (except those "for convenience" that are really healthy). But if women are dying because surgeons want work, and they can bill the insurance company or government that is just not right on all levels. Of course all your risks increase when surgery is involved whether you are healthy or not. Turns out the women in that group, remember where one in 3,000 die during childbirth that are NOT high risk pregnancies, but healthy ones with no signs of a problem. Yes, there could be one, but chances will be much lower than in high risk birth. Number one priority is always the health of the mother and baby with a doctor or nurse midwife, and that is exactly my point. If we really want to take care of these women we need to improve the systems for determining if a C-Section is needed or not. Sure doctors to the rich and famous are making money catering to those mothers that can afford to order a C-Section if they want, but there will always be a risk with that group as well because its surgery and people's bodies react differently under those conditions. Letting all groups know that a C-Section should be avoided not "ordered for convenience" could save lives. What a tragedy. An event that is supposed to bring joy and happiness, ends in death and possibly a child without a mother and a husband/partner alone. Performing this surgery in healthy women when it can be avoided is something hospitals, doctors, and midwives can do all across the country and around the world to save lives and precious healthcare dollars. We need to start looking at our healthcare dollars in a different way. Each one of those dollars could save a life. If it is spent wisely, it could save two lives instead of just one, and possibly more because that dollar prevented a much bigger, more expensive healthcare event from happening. With a world population of seven billion people, where it took all of mans history until 1800 to reach one billion, and if you apply the power of doubling, our next billion could happen in just a few years. If we don't want to lose our freedom to have as many children as we want, something has to change fast. We have to find a way to support and feed the future children of the world with limited resources. If we don't figure it out now while we have choices, the suffering and fighting for rights to things like farmland and water will be dominated by big corporations like Monsanto that have already set their sites and invested their dollars toward control of just these things. Control the food and water and you control the people. We have to take control of the problems we face, and solve them together as a world. Let's make it a competition and identify industries that support making sure that people have affordable access to food, shelter, water, and healthcare because with are kicking butt with industries that support people taking local control. If you think about it, more local control and ability to survive off the grid makes us stronger not weaker. That is what these industries don't want us to get a taste of because they have built an industry around an intrastructure that is being obsolete. The costs for global warming could go far deeper than we ever imagined. Industrial agriculture that is built on a system of GMOs, pesticides, and using the soil like a prostitute is responsible for pumping billions of tons of carbon into the air where organic farming sequesters carbon, uses less water, and by year three has higher yields. Coal is so big and responsible for so much of the pollution we need to look at getting rid of it or they better take those billions in profit and fit a way to clean it up. Problem is owners (some owners have huge chunks of the business) really have no motivation to even start because no one is making them. Obamas efforts to put restrictions were changed just a few weeks later. Disappointing to those that understand the significance in getting that industry to do anything. Wise use of our healthcare dollars is something we are passionate about at Smart Health Talk, because the potential to save billions in wasted dollars is there. Would rather eliminate unnecessary C-Sections or prevent a case of diabetes from even happening at all and use the money for a surgery that would be denied by an insurance company because they don't want to fork up the money and the patient gets a death sentence when they could live if they had the treatment. Don't want to be part of a system that does that to feed corporate pockets. When healthcare is a profit based business it gives corporations permission to play God. Wasteful use of healthcare dollars and unnecessary death because of poorly designed heathcare systems is something that can be changed with healthcare reform efforts. Take a model that works and duplicate it. Offer incentives for "first visits" to get people started that may not have been to a doctor in years. According to second article below, "Curbing C-sections could save countries billions," if we could most importantly concentrate on not performing that first C-Section. After having one C-Section the need to have a mandatory C-Section for all subsequent births can possibly be avoided. Once a woman has had one C-Section she is now considered a "high risk birth" and to protect themself from a malpractice suit, an obstetrician would want to do the C-Section instead of trying to help the woman deliver vaginally. There were midwives that had told me how some of their patients were these women. They had been either sucked into a previous C-Section when it could have been avoided, or had a life threatening situation that required the surgery with a previous birth. Doctors had told her they did not want to support her choice, and it was important to her to have that with the new baby. For certain women, they felt they had been deprived of that part of the childbirth experience. As for my experience of delivering both my children at home with a my midwife, they will always be some of my most special memories. Yes it was painful without drugs, but your body makes its own drugs and can give you an out of body experience in the process. My midwife reminded me that with each contraction you are getting closer to seeing your baby's face, and you can get through it. After weeks of coming to classes on childbirth and exams with your midwife, you develop a special bond and trust like no other. Her voice becomes part of the drug that helps you make it through it. I didn't want my babies to come into the world drugged up. It paid off when I had my first moment alone with my son in my bed, in my house not long after he had been born. I held him, looked into his eyes and told him how much I loved him. He then got this big smile on his face like he could feel the energy from my voice. Don't think that would have happened that way for me in a different setting. There were a couple of other things that worried me about having my baby in a hospital. Wanted to avoid hospital bacteria that carry sicknesses that you get just by being in the hospital. Didn't want my baby exposed to a building full of sick people. Wanted to keep the rhythm of the contractions steady. It was that rhythm and the extraordinary skills of my midwife that kept me from having to use the hospital plan. You think of a lot of things when preparing for childbirth, but the rhythm of the contractions is usually not one of them. They hit you like nothing else. Where a scratch is an outside pain that projects in, a childbirth contraction is a pain that starts for your core and projects out. You cannot escape it. The only choice is to embrace it, and tolerate it. The thought of the millions of women that have made it through the pain, and how you get to join that group of women that experienced every sensation of childbirth helps you somehow. We stood, we walked, and used a birthing chair. Never was I on my back pushing. Only standing up and making good use of gravity. Had no desire to lay down, and would have been miserable. If not for the midwife, my delivery would have probably been a C-Section. She used techniques midwives have been using for thousands of years to save the lives of women with no hospital to go for an emergency. With each contraction she used her fingers to open my cervix that was not dilating. There may be doctors that would do that, but don't think there are many. Maybe they should learn as part of their job because it works and save upwards of $35,000 a pop when maybe you could help pop that baby out the way nature intended. If people have their own money for the "convenience births" and doctors are willing to do them, that's their right, but may want to look at the 1 in 3,000 deaths to healthy mothers by having a C-Section surgery. Some may even elect to have the surgery to have their tubes tied and a tummy tuck since you sliced me anyway. That actually makes sense in that it could avoid another surgery. The biggest risk to the baby is asthma or trouble breathing and is more prevalent in premature babies. For someone that was determined to only have surgery as a last resort, I was grateful for what she did for me. As for my experience with delivering both my children at home with a my midwife, they will always be some of my most special memories. Yes it was painful without drugs, but you body makes its own and can give you an out of body experience in the process. My midwife reminded me that with each contraction you are getting closer to seeing your baby's face, and you can get through it. After weeks of coming to classes on childbirth and exams with you midwife, you develop a special bond and trust like no other. We stood, we walked, and used a birthing chair. Never was I on my back pushing. Only standing up and making the use of gravity. Had no desire to lay down, and would have been miserable. If not for the midwife, my delivery would have probably been a C-Section. She used techniques midwives have been using for thousands of years to save the lives of women with no hospital to go for an emergency. With each contraction she used her fingers to open my cervix that was not dilating. There may be doctors that would do that, but don't think there are many. Maybe they should learn as part of their job because it works and save upwards of $35,000 a pop when maybe you could help pop that baby out the way nature intended. If people have their own money for the "convenience births" and doctors are willing to do them, that is their right, but may want to look at the 1 in 3,000 deaths to healthy mothers by having a C-Section surgery. Some may even elect to have the surgery to have their tubes tied and a tummy tuck since you sliced me anyway. That actually makes sense in that it could avoid another surgery, but would have to know the increased risk to the baby. For someone that was determined to only have surgery as a last resort, I was grateful for what she did for me. UnneCesareans: Documented Causes of a Disturbing Trend

GreenMediaInfo.co
Posted on: Tuesday, November 6th 2012 at 5:00 am Written by: Judy Cohain, CNM Abstract: A recently coined term, unneCesareans, describes the mode of delivery for 25% of low-risk first births in most Western countries. Evaluation of Cesarean Delivery,published by the American College of Obstetricians and Gynecologists (ACOG) showed a lack of evidence of improved medical outcomes with the widespread use of cesareans for low-risk, full-term first births, therefore, they are medically "unnecessary". Eighteen causes for this common practice have been documented in published research. Since UnneCesareans have multiple causes, a reverse in current trends is unlikely. When I tell people that I am a homebirth midwife, they often respond by asking, "Why do women choose to give birth at home?" It would be wonderful if the answer would be that hospital outcomes are comparable to attended homebirths and homebirth is just more comfortable. But since US hospitals delivered 32% of low-risk women by cesarean surgery since 2007 and 1 in every 3000 of those died from the surgery, the answer is simple: to avoid dying in childbirth or being scarred for life by unnecessary surgery. Then, the second question the listener naturally asks is, "Why do doctors do unnecessary surgery?" Many doctors and midwives are also concerned with this question and have researched it extensively. The following is a review of the recent research, most of it published since 2006, regarding the causes of unneCesareans. 1. Provided free (or covered by insurance) everywhere but New South Wales, Australia: In 2007 the Department of Health of New South Wales, Australia, passed Policy Directive #2007-024, demanding that "maternal request is not an indication for elective caesarean section." Compliance with the directive is mandatory and a condition for subsidy. However, no other government in the world distinguishes between unneCesareans and medically indicated cesarean surgery. 2. Private medical practices: The consummate example of this is in Brazil, where the cesarean rate in a private hospital among primiparous women was 97.8% vs. 47% in public hospital.(1) 3. High socioeconomic level of the pregnant woman.(2) 4. Highly urbanized setting.(3) 5. Physician convenience: Weekday, day shift: 66% of emergency cesareans took place between 8 am and 3 pm, and not a single one between 5 am and 6 am.(4) UnneCesareans are not performed on weekends or national holidays, in order to not interfere with leisure time.(5) 6. Action Bias: Doctors and judges exhibit an action-bias towards cesareans. Surgery is considered by the courts to be heroic and the ultimate effort, regardless of the outcome—even death. No one gets sued for doing a cesarean, only for not doing one.(6) 7. Dystocia has no medical definition: The most recent ACOG Practice Bulletin on dystocia specifies no time frame for dystocia, referring only to slower than "normal" or complete cessation of progress, allowing doctors to define it arbitrarily. (7) This undefined phenomenon of "dystocia" is held responsible for between 50% and 70% of all cesareans experienced by otherwise healthy nulliparous women.(8) An example of an arbitrary but frequently applied definition of dystocia is giving women with an epidural in place an extra hour to give birth before defining them as having "second stage dystocia."(9) Even so, the strongest risk indicator for dystocia was use of epidural analgesia.(10) 8. Elective Induction: Lowe reported a 1.5 to 2.5 times greater risk of cesarean in nine controlled international studies using large samples of healthy first births at term with a singleton cephalic pregnancy with elective induction. The primary indication for cesarean was dystocia.(11) 9. Overeating high glycemic index foods combined with lack of exercise: About 10% of fetuses weigh over 4000 g (approximately 8 lb, 13 oz).(12) Mulik reported an overall cesarean rate of 16.4%.(13) Full-term, cephalic pregnancies not complicated by any medical or surgical disorders—with the exception of 0.5% gestational diabetics with birth weights of 2500–3999 g (about 5 lb, 8 oz to 8 lb, 13 oz)—had a cesarean rate of 14.7%, but babies born weighing over 4000 g had a 30% cesarean rate and those over 4500 g had a 60% cesarean rate. Therefore, in this study, a 9% rate of macrosomia was demonstrated to increase the overall cesarean rate from 14.7% to 16.4%, or an addition of 1.7%. Birth weights of 2500–3000 g can be achieved by avoiding high glycemic index foods combined with daily exercise.(14) 10. High and rising malpractice insurance premiums and lack of caps or limits on payments for non-economic damages: Multivariable analyses demonstrated that for each annual $10,000 insurance premium increase, the primary cesarean birth rate increased by 15.7 per 1000 for nulliparous women and 4.7 per 1000 for multiparous women.(15) A $10,000 decrease in premiums for obstetrician-gynecologists would mean an associated decrease of 0.15% in the rates of primary cesarean section and an increase of 0.35% in the VBAC rate. Two types of tort reform caps on non-economic damages and pretrial screening panels were associated with lower rates of cesarean section and higher rates of VBAC.(16) 11. Breech/VBAC cesarean section protocols do not differentiate between small and large fetuses: Vaginal breech delivery of 2500 g is safe. Breech delivery of 4000 g is risky. VBAC of a 2500 g baby is associated with the low uterine rupture risk of 1 in 1000, smaller than the risks of repeat cesarean section. VBAC of a baby over 4200 g has a risk of uterine rupture of 1 in 50.(16) Current protocols do not take fetal weight estimations into consideration for the purposes of avoiding cesarean or repeat cesarean. Manual and ultrasound fetal weight estimations are considered reliable enough to justify cesarean when the baby is big but are not used to justify avoiding cesarean when the baby is small. 12. Epidurals: Randomized trials that do not show an effect of epidural anesthesia on cesarean section rate lack external validity.(17) The limited data available suggest that epidurals and low-dose oxytocin used together increase the cesarean section rate.(18) High dose oxytocin is associated with less cesareans but more uterine ruptures. 13. Longer hospitalization and re-hospitalization is more likely and more profitable: After a planned primary cesarean, women were 2.3 times more likely to require a re-hospitalization in the first 30 days postpartum.(19) The average initial hospital cost of a planned primary cesarean was 76% higher than the average for planned vaginal births and length of stay was 77% longer (4.3 days to 2.4 days). This creates more profit if the hospital is reimbursed per day.(20) 14. False claims that maternal request cesarean section is popular: Existing evidence for large numbers of women requesting cesarean sections in the absence of medical indications is weak.(21) 15. Continuous fetal monitoring of labor of low-risk pregnancies: Continuous cardiotocography (electronic fetal monitoring in the US) was associated with a significant increase in cesarean section. There was no difference in the number of babies who died during or shortly after labor, and no difference in the incidence of cerebral palsy.(22) 16. Lack of hospital-provided doulas: For middle-class women laboring with the support of their male partner, the continuous presence of a doula during labor significantly decreased the likelihood of cesarean birth.(23) 17. Midwifery model of care replaced by risk-focused, policy-driven, non-woman-centered care: Studies with Certified Nurse Midwives and Certified Professional Midwives have found that intended home and birth center births for low-risk women have significantly lower cesarean rates than for comparable low-risk women in hospitals with equally low infant mortality.(24) 18. Lack of practitioners with 90% success rate at external cephalic versions. Summary"Caesarean sections, unless strictly indicated, may be harmful to the health of mothers and their newborn babies. Two questions remain. Why are rates still on the increase? What can be done to reverse current trends?"(25) As a head obstetrician recently said, "If highly-paid soccer goalies won't practice evidence-based diving for the ball when they are paid millions of dollars a year, what hope is there for obstetricians?"(26) UnneCesareans have multiple causes and therefore, a reverse in current trends is unlikely.http://www.greenmedinfo.com/blog/unnecesareans-documented-causes-disturbing-trend Curbing C-sections could save countries billions

By Amy Norton
Reuters NEW YORK | Fri Mar 23, 2012 2:36pm EDT (Reuters Health) - Putting a halt to medically unnecessary cesarean sections could save more than $2 billion a year worldwide, a new study estimates. It has long been recognized that many countries have high C-section rates. In the U.S., C-sections now account for one-third of all deliveries -- an all-time high. The reasons are various. The rising rate of multiple births has played a role, since twins or "higher-order" multiples often need to be delivered by C-section. But experts generally agree that rates in the U.S. and many other countries are too high, since it's unlikely that the rapid increase since the 1990s is due exclusively to medical need. There is no agreement on what the "correct" C-section rate is. But the World Health Organization has suggested that rates above 15 percent are probably too high. In the new study, researchers found that 69 countries worldwide top that 15 percent rate. On the other end of the spectrum, 54 countries had C-section rates lower than 10 percent -- which may be below what is medically needed. Then the researchers calculated the costs. In countries with high C-section rates, they estimate, getting the figure down to 15 percent would save $2.3 billion globally each year. In countries with low rates, the cost of bringing them up to 10 percent would be $432 million, the researchers report in the American Journal of Obstetrics and Gynecology. The findings paint a picture of the global "inequities" in C-sections, according to Drs. Jose Belizan and Fernando Althabe, who worked on the study. One implication is that a "better distribution" of resources could allow more women in poorer countries to get medically needed C-sections, said Belizan and Althabe, of the Institute of Clinical Effectiveness and Health Policy in Buenos Aires,Argentina. Recruiting professionals from high-rate countries to perform C-sections in low-rate ones -- or to train local health providers to perform them -- is one possibility, the researchers said in an email. Still, putting a dollar figure on the savings from reducing unnecessary C-sections is tricky. One issue is that this study assumed that the correct C-section rate is no higher than 15 percent. "And that is a very debatable point," said Dr. George Macones, who heads obstetrics and gynecology at Washington University in St. Louis and chairs the Committee on Obstetric Practice for the American College of Obstetricians and Gynecologists. "While cost is one factor to consider," Macones told Reuters Health in an email, "I think that we should be most concerned about doing what is in the best interests of our patients." There are other reasons to limit C-sections to only those cases where it's the best course for the mother's or baby's health. Although the procedure is generally safe, it is still major abdominal surgery with inherent risks, like infection or too much blood loss. C-sections also boost the odds of certain problems with later pregnancies, including abnormalities in the placenta that can lead to severe bleeding during labor. According to Macones, a number a factors have likely driven the rise in the U.S. C-section rate. Some women request the procedure, for instance, so as to choose when they give birth or to avoid long labor. And obstetricians may be quicker to do them now than in years past. Worry over being sued should something go wrong during natural labor and delivery is one factor, according to Macones. But he said there are potential ways to bring the C-section rate to a more appropriate level. "I think the most important is to try to avoid first cesareans, and do them only when indicated," Macones said. One way to do that, he added, is to limit labor inductions to only cases where they are necessary. In inductions, doctors use medication or instruments to stimulate labor. But if labor fails to progress normally, a C-section may become necessary. Another way to limit C-sections, Macones said, is to do more vaginal deliveries in women who've had a C-section in the past. Repeat C-sections account for a large share of the U.S. total, even though experts say many women can successfully deliver vaginally after a past C-section. There is a chance the C-section scar will tear during labor, but it's rare. Still, many U.S. hospitals do not offer those women the option of a vaginal delivery because they cannot guarantee a team on hand to perform an emergency C-section if necessary. Just how to curb high C-section rates remains the "million dollar question," Belizan and Althabe said. But Macones noted that last year, U.S. officials reported the first dip in the national C-section rate in more than a decade. In 2010, the rate was 32.8 percent, versus 32.9 percent the year before. Not a dramatic difference, but experts were hopeful that it pointed to a leveling off. As for poorer countries, Belizan and Althabe said there are numerous obstacles to women getting needed C-sections. High rates of home birth, too few hospitals and too few providers who can perform the surgery all remain barriers. SOURCE: American Journal of Obstetrics and Gynecology, online March 5, 2012. http://www.reuters.com/article/2012/03/23/us-cesarean-idUSBRE82M0Z020120323
Research Links Phthalates to Type 2 Diabetes
|

Avoid plastics that do not have the recycle #1. The products with #1 are safer for your family.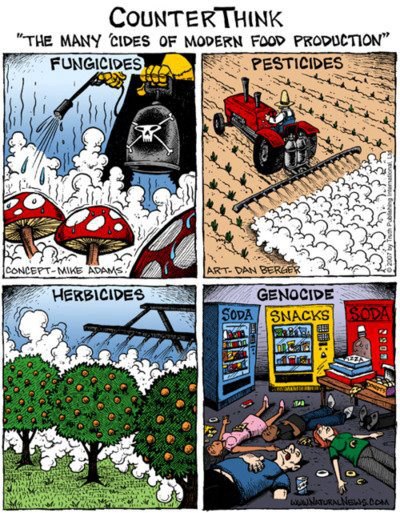
aka “Fragrance,” “The Softener”
Phthalates like to make hard plastics more flexible, and to act as an adhesive, dye, and solvent in other products. Phthalates don’t care about fame — they prefer to stay hidden on product labels with simple pseudonyms like “fragrance.” Phthalates may be publicity shy, but given the right setting, they can off-gas and volatize with the best of them. Air fresheners contain phthlates.
How to avoid
1. There’s no sure-fire way to completely avoid phthalates until Congress passes the Safe Chemicals Act, legislation that will require chemical manufacturers to demonstrate that their products are safe before they end up in our lotions, dashboards, and bodies. Until then... 2. Skip the fragrance when choosing cosmetics, personal care products, cleaning products, detergents, and air fresheners. Manufacturers aren’t required to list phthalates on the label, but any item listed as “fragrance” is often a chemical mixture that can contain phthalates. 3. When buying cosmetics, purchase from companies that have pledged not to use phthalates. 4. Check the Healthy Toys database for toys bought before 2009 - they may contain phthalates. 5. Avoid buying plastics that may be treated with phthalates, including vinyl toys, shower curtains, and gloves. Look out for "PVC," "V" or the "3" recycling code on the item or its packaging.
6. If you have vinyl flooring in your home, damp mop regularly since phthalates bind to dust on the floor. Direct sunlight on vinyl tiles causes them to release phthalates more quickly, so put lower blinds on windows that shine directly on flooring.
Frequent hangouts Cosmetics and personal care products; fragrances used in products ranging from cleaning products to perfumes and air fresheners; pharmaceuticals, medical devices, toys, food packaging, sealants, printing inks, vinyl shower curtains, and building materials such as vinyl flooring, house dust. Why they're dangerous Phthalates are linked to lower testosterone levels, decreased sperm counts andpoor sperm quality. Exposure to phthalates during development has been linked to malformations of the male reproductive tract and testicular cancer. Young children and developing fetuses are most at risk. Phthalates also have been associated with obesity, reduced female fertility, preterm birth and low birthweight, a worsening of allergy and asthma symptoms, and behavior changes. Fun fact Enjoy that new car smell? Thank phthalates! Because phthalates are not chemically bound to products, they easily migrate or off-gas, making them easy to inhale. 
Plastic bottles can contain phthlates. Only choose bottles with the #1 recycle code. Avoid all bottles with the #7.
Visit our account for more graphics:
|




|
|
|
|